Table of Contents[Hide][Show]
If you’ve noticed shifting in your teeth, having bite issues, or wondering if braces are a good decision, you may have questions about braces.
Whether you have dental braces now or they’re an option you’re considering, here’s a comprehensive guide on what kinds of braces are available, what to expect, and how to care for them.
What are braces for teeth?
Braces for teeth come from a special field of dentistry called orthodontics. This area of dental work was developed to treat problems with the positioning of the teeth and jaw. Even though each mouth is different, several bite issues necessitate orthodontic treatment.
The first type of problem we encounter is malocclusion, or bite misalignment. The most obvious forms of this issue is what we know as an underbite or overbite. However, many other forms of malocclusion can occur.
Overcrowding, spacing issues, missing or crooked teeth, an overjet, or even an open bite can also occur as teeth grow in. Unfortunately, these conditions can cause patients to be self-conscious. Worse, these problems can affect eating, smiling, and even speaking.
Good news—while there are many forms of bite issues, there’s always a solution to these misalignments.
Braces were developed to bring the teeth and jaw into proper alignment, so there’s hope for your malocclusion woes. In fact, this treatment has an overall high satisfaction rate and effective results.
You may notice a bite problem on your own, or a dentist may point it out during a visit. Once a malocclusion has been diagnosed, you have many options in the world of braces.
Get Dr. B’s Dental Health Tips
You can’t be healthy without a healthy mouth. Sign up for my free newsletter and you’ll get my unconventional tips, starting with: If I had a cavity, here’s exactly what I’d do to reverse it.

Types of Braces
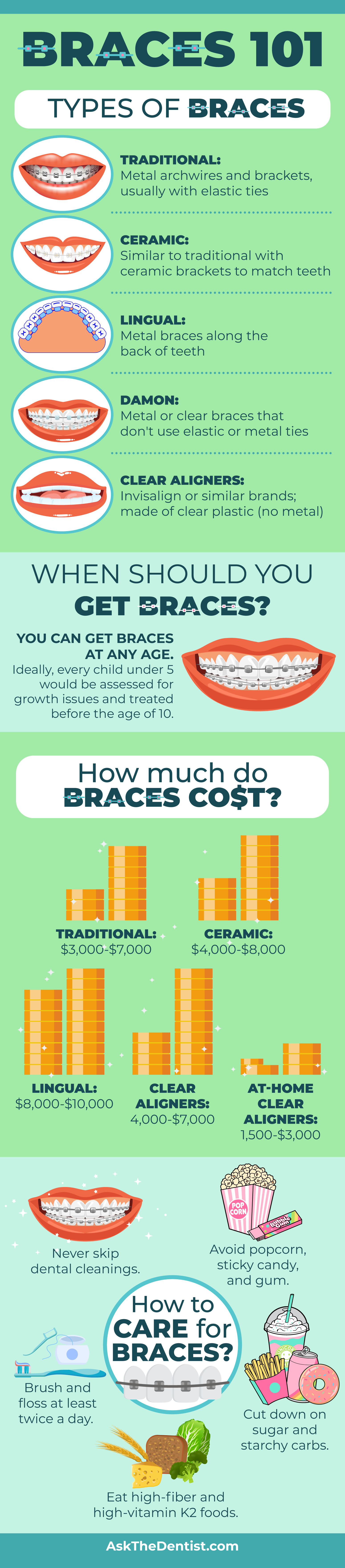
Today, there are more types of braces available than ever before. These options leave many patients wondering, “Which braces are right for me?” That answer and resulting treatment plan can depend on everything from cost to appearance. The pros and cons of each type of braces can help you decide which variety suits you best.
1. Traditional Metal Braces
These are the classic variety of braces that most people think of when they hear the term. This option shifts alignment using metal brackets attached to the front of the teeth. The teeth are guided by an archwire that slowly repositions the bite.
Some braces utilize elastic ties to support the movement of teeth, while self-ligating braces have a custom-made clip that replaces elastic ties.
For patients allergic to nickel, the metal used in traditional braces might cause concern. Not to worry! Alternative options are available, such as gold-plated stainless steel or titanium. Be sure to discuss any metal allergies with your dental care provider before taking the plunge.
- Pros: fun color choices for kids, usually have the lowest price point, fast-acting
- Cons: most conspicuous choice, white calcifications can develop around brackets
2. Ceramic Braces
Ceramic braces are similar in appearance to traditional metal braces. However, there’s one major exception—the brackets are clear or match the individual’s teeth. This provides similar treatment to metal braces, but without a metallic mouth look that might deter some patients.
- Pros: less obvious than traditional metal braces, act much faster than other clear options like Invisalign.
- Cons: staining is very possible due to the light color, higher cost than the metal option, calcifications are possible
3. Lingual Braces
Dental professionals refer to the inner side of your teeth as the “lingual” surface. These braces are located on the back of the tooth, against the tongue. Lingual braces are made of metal, like traditional models.
- Pros: not visible in everyday wear
- Cons: tough to clean thoroughly, higher cost than regular metal braces, can hurt teeth and tongue in early months, not an option for severe malocclusions, adjustments are more frequent and complex
4. Damon Braces
These are a newer option for braces that don’t use the elastic or metal ties of traditional braces. Damon claims to reduce pain and require fewer adjustment visits than a classic model. This option comes in both a metal bracket and clear version.
- Pros: Damon claims faster treatment times, less conspicuous than traditional metal braces, and less pain than braces that need to be tightened
- Cons: relatively new method, not all orthodontists offer this option, higher price point
5. Clear Aligners (Invisalign)
Clear aligners are potentially the mildest option out of the types of braces. However, don’t be fooled by these clear braces: they can accomplish great results over time.
Each aligner you’re given is choreographed for just 1-2 weeks at a time, gently moving your teeth to the desired position.
Patients with interproximal reduction or severely rotated teeth will not be good candidates for at-home treatment (like SmileDirect or Candid), but they can almost always get their desired results when using Invisalign under the care of a dentist or orthodontist.
- Pros: almost invisible, easily removable, no calcifications, and use safe and patented plastic (free of BPAs and carcinogens)
- Cons: higher price, process may take longer, easier to lose with costly replacement fees
At what age should you get braces?
One downside of beginning treatment in your adult years is that it will likely take about twice as long to get results.
That’s why I advise parents to consider orthropics, a school of orthodontic thought that seeks to correct growth issues starting as early as two years of age.
Orthropics has an emphasis on prevention and also strongly avoids extracting teeth.
Professionals separate orthodontics into Phase 1 and Phase 2 treatments. In an ideal scenario, a child would receive an orthodontic and orthotropic consultation between the ages of two and five, in Phase 1. From there, they would receive monitoring and any necessary adjustments between ages 4-10 to optimize jaw and palate growth.
Phase 2 treatment refers to orthodontic treatment stated during or after early adolescence. If Phase 1 treatment has been completed, it can reduce or eliminate the need for orthodontics in this stage. However, if you missed out on early intervention, don’t worry. Age should never prevent you from getting the treatment you need.
While it’s clear from the data that earlier orthodontic intervention yields better results, it’s never too late. Though your bite may not have the same flexibility and responsiveness as you age, change is still possible.
Living with a malocclusion can increase your chances of bruxism, make brushing and flossing harder, and impact your confidence. Even if early treatment is no longer an option for you, there’s hope.
How Dental Braces Straighten Teeth
Not all braces straighten teeth the same way, but all are working toward the same goal of aligning the teeth and jaw. The type of braces you choose determines the way your teeth are straightened. It will also establish the frequency of adjustments needed throughout the process.
Though some components can be changed to suit individual needs, the basic mechanisms are the same. Here’s how the many parts of braces work together to straighten teeth.
Brackets
Brackets are cemented to each tooth and may be metal, tooth-colored, or ceramic. These can attach to the front or back of the tooth, depending on if the braces are traditional or lingual. Bands that wrap around the tooth are put on the back molars in some cases, while self-ligating braces don’t require rubber bands.
Wires, Tubes, and Ties
Archwires are attached to the brackets and will guide the teeth as they move. This wire applies steady pressure to the jawline and teeth, slowly moving their position. The archwire is adjusted to continue to realign the teeth and jaw throughout the treatment period.
The orthodontist will fasten archwire to the brackets using small rubber or metal ties, which they will change periodically. A small tube holds the wire in place at the last tooth on each side. In more serious cases, rubber bands, elastics, or springs may be necessary.
Movement
These pieces all work together to move the teeth into alignment, and to shift the bite into its proper placement. As the teeth move, guided by the arch wire, the brackets act like little handles to assist in pulling the teeth along. As the braces are tightened during regular adjustments, the teeth and jaw continue on this path.
Damon Braces
This method is similar in some ways to traditional braces, but with a few modern changes. Damon braces do not use metal or elastic ties, and treat alignment issues without needing to be tightened. Instead, their shape-memory wires create movement, and they are self-ligating.
Clear Aligners (like Invisalign)
These models work a little differently. Unlike other forms of braces, a clear aligner is removable and provides a gentler adjustment. Instead of regular visits to tighten the archwire and ligatures, a new aligner is used every two weeks to continue moving the teeth.
Headgear
In more severe cases, headgear may be needed. This removable gear typically attaches to the upper back molars in order to correct jaw alignment and create more space in the teeth. While this one of the largest orthodontic appliances, it’s rarely necessary and can typically be worn at home to prevent self-consciousness.
Getting Braces: What to Expect
Getting braces isn’t a mysterious process, and knowing what to expect can calm your nerves. Here’s what’s in store before, during, and after getting braces for your teeth.
Before
Before you get braces, there are some important preparation steps to take.
I never advise braces until all decay and gum issues, like cavities or gingivitis, have been addressed.
If left untreated, these can cause major problems down the road that could undo the progress your smile has made through braces.
In some cases, surgery may be required for braces. Orthognathic, or jaw, surgery is occasionally needed for more serious alignment issues. Your dentist or orthodontist will let you know if you need this step to correct TMJ, jaw closure problems, facial imbalances, or other concerns.
Palatal expansion or serial extraction may also be necessary if teeth are overcrowded. This measure works best in Phase 1 because the growth plates in the mouth are still developing at this age.
This process may look different for adults or adolescents since their palate is formed. These patients may need teeth pulled to make space for proper alignment, or spacers put in between teeth to make room for bands before braces. Spacers and expanders may cause some soreness, but it’s not long-lasting.
Once the mouth is ready for treatment, your orthodontist will take x-rays and photos of the teeth. These images will guide them in designing braces to fit your individual needs. They will also take an impression (or mold) of your mouth to ensure a good fit when the braces are put on.
During
So now that you’ve cleared up any tooth decay or gum issues, pulled teeth or expanded the palate if needed, and prepared with your orthodontist, it’s time to finally put on those braces! The good news is that this typically only takes as long as a movie—1 to 2 hours. Having your braces put on can take one or two visits, depending on the type you’ve chosen.
Braces are made to fit you individually, so no two cases of putting on braces will be exactly the same. However, the procedure for traditional metal or ceramic braces typically follows these steps:
- Cleaning: a proper cleaning and drying will occur before any braces are put on.
- Brackets: each tooth will need a bracket placed in the center, which will be held in place by glue. Your orthodontist will place the glue on the tooth, dry it with a blue light, and then apply the bracket. Don’t worry if the glue tastes a little unpleasant; the taste is only temporary.
- Bands: these help to secure the braces in your mouth. These bands will be slipped around the back molars on both the upper teeth and lower teeth. The bands are secured with glue and chosen based on your impression, and you may feel some pressure as they are secured firmly. Let your orthodontist know if you feel any significant pinching, as they may want to readjust the band to a more comfortable position for you.
- Archwires: you’re in the home stretch! These are the last step in putting on your new braces. The orthodontist will attach these metal wires to your brackets using a rubber band. If you are using traditional metal braces, you can choose the rubber band color, but ceramic braces will use ligatures that are clear or tooth-colored.
Lingual braces are applied in an extremely similar way, but to the inner side of the teeth. This requires more time and a specially trained orthodontist to ensure proper care.
Invisalign and other clear retainers are a very different form of braces. For more information about how they are put on and what treatment might look like, check out my guide to Invisalign.
While each mouth is an individual case with individual needs, there are a few things I always recommend doing during your dental braces treatment:
- Try remineralizing toothpaste. While most people are familiar with fluoride toothpaste, I recommend the road less traveled: hydroxyapatite (Ha or NHa) toothpaste. This can help remineralize teeth, which means rebuilds enamel and reversing tooth decay. Fluoride can have some undesirable side effects, but remineralizing toothpaste doesn’t share those same potential drawbacks. (I love this toothpaste; use code ASKTHEDDS for 10% off.)
- Avoid alcohol-based mouthwash. Traditional mouthwash can kill the good bacteria in your mouth, lead to overgrowth of bacteria that can damage your teeth, and pave the way for inflammation and decay. On the other hand, an oil pulling mouthwash like this one can do more good than harm.
- Mouth tape for nighttime protection. Many people breathe through their mouths at night, and it can wreak havoc on your oral health. Mouth taping prevents the growth of harmful bacteria, improves your sleep and gut health, and boosts immune response.
- Brush and floss intentionally. Brush your teeth in the morning, before bed, and 30-45 minutes after any meal that contains decay-promoting foods. Braces can act like a magnet to food and bad bacteria.
As we’ve discussed, braces work by guiding the teeth along the wires into their healthy new position. With traditional metal braces, ceramic braces, or lingual braces, you will need to see your dentist every 3-6 weeks for an adjustment to keep moving your teeth along their journey.
This will involve tightening the wires, springs, or elastic bands on your braces to increase the tension and continue to shift the teeth and jaw into correct alignment. After these visits, you may experience some soreness as the teeth move into their new position.
After
Removing your braces is much less painful and time consuming than putting them on.
Your orthodontist will remove the brackets and bands, and snip the archwire. It’s common to need the glue removed, and your dentist may polish it off with a special tool. This process is relatively quick and you should only feel a little pressure.
S/he will also take new photos and x-rays to see how the mouth has changed. This will help them in future treatment and show you how your teeth are aligned. At this stage, you’ll probably want to show off your beautiful smile and malocclusion-free mouth.
You’ll also be given a new retainer. Be sure to wear your new retainer consistently to keep the results you worked so hard for. If your teeth aren’t quite ready for a retainer, a pre-finisher may be advised first.
Rarely, surgery will be needed after braces for optimal results. Some patients need headgear after braces. Others will need a fiberotomy to prevent their teeth relapsing and rotating, or a gum lift to ensure the teeth are uniform after being moved.
Pain with Braces: What’s Normal, What’s Not
Braces may not always be comfortable, but they should never be seriously painful. The most common times to experience soreness are after an adjustment and the first several days after braces are put on.
Over the counter pain relievers can help, but my favorite recommendations are CBD oil, coconut water, or clove oil. Their anti-inflammatory properties may help control these symptoms, and the pain should lessen as time passes.
If you are experiencing severe pain, contact your orthodontist. It’s possible for a wire to be pushing into your gums, a bracket to be loose, or other concerns. Also, if you are consistently experiencing high levels of pain after an adjustment, be sure to communicate that as well. Your orthodontist may be able to alter the way s/he adjusts your teeth to put you at ease.
Braces Cost (by Type)
The pricing of braces is determined by the length, amount, and type of orthodontic treatment needed. Also, braces can cost less depending on what part of the country the orthodontist is located in, and if they’re based in a rural or urban area.
- Traditional metal braces: $3,000-$7,000
- Ceramic braces: $4,000-$8,000
- Lingual braces: $8,000-$10,000
- Clear aligners: $4,000-$7,000
- At-home clear aligners: $1,500-$3,000
Some costs happen up front. X-rays range from $50-$250, while an initial consultation with the orthodontist can commonly run up to $200. After treatment, a retainer can cost anywhere between $150 and $1,000, depending on the type you get.
Does insurance cover braces?
It depends—some types of medical insurance cover braces only if they are medically necessary, such as for restoration after a major incident. It’s common for some dental insurance plans (if orthodontics is included) to pay for 50% of braces and cap at $1,500 total per child. Most plans won’t pay for braces for adults over 18-21 except in special circumstances.
However, all plans are different, so be sure to speak to your provider.
If you’re reeling from sticker shock, there’s good news. Braces can typically be broken down into installments at most orthodontist’s office. Also, if the braces are medically necessary, they should be tax deductible.
Look for more tips on saving on dental care in my article on living with no dental insurance.
How to Care for Your Braces
Eating with Braces
What you eat can make or break your braces…sometimes literally.
Popcorn, sticky candy, and gum can pull a bracket or wire free from their carefully placed alignment. Furthermore, don’t eat foods that will promote decay while your have braces, especially since the teeth will be harder to clean.
This includes sugar rushes such as sweets and soda, and carb-loaded treats like bread and pasta.
You should also eat foods that promote your oral health. Diets like Paleo and keto are full of foods that your teeth and gums will love. This eating plan can help remineralize your teeth and reduce gum inflammation from the inside out.
Problems with Wires or Brackets
If you encounter any orthodontic problems with wires or brackets, let your dentist know right away. They can give you an adjustment to fix any wires of brackets that have detached or shifted.
In the meantime, try dental wax, which is made to put on protruding wires or brackets in a pinch.
For immediate relief, be sure to wash your hands and pinch off a pea-sized portion, then apply the wax to the fixture that’s prodding you.
Wearing Retainers After Braces
Once the braces are removed, you’ll need to wear a retainer to ensure your teeth stay where they are. It’s crucial to wear your retainer at least 22 hours a day for the first year, then nightly for the rest of your life.
Otherwise, your teeth may shift back to their original position, causing you to lose your hard-earned results!
Sometimes, an orthodontist may recommend a bonded retainer, which is a metal retainer permanently bonded to the backside of the teeth. I generally advise against these for most patients, as they collect tartar and calculus and make flossing harder.
Pro tip: check out my handy guide on how to clean retainers to get the longest life out of yours.
How to Brush and Floss with Braces
It’s not surprising that braces can make brushing and flossing more difficult; braces can add a lot to navigate around while practicing oral hygiene. Taking special care to keep your teeth pristine during the process can save you from developing decay and gum inflammation.
I recommend a sonic toothbrush as my toothbrush of choice for patients with braces.
My favorites are the Philips Sonicare DiamondClean and Fygg.
When brushing, take special care to brush around brackets, wires, and bands. These can harbor plaque, tartar, and food particles, and need particular attention.
Flossing is a bit trickier with braces. Here’s how to do it:
Thread a piece of waxed floss under the archwire before gently and gently move it up and down. Once finished, pull it back out through the wire and move on to the next tooth.
Still having issues? Try a water flosser like Waterpik, dental tape, or a floss threader.
While this process may feel tedious, it will save you from major dental work down the road if your braces lead to decay.
Braces Before and After
Want some examples of what results you might expect with braces? Check out these success stories.
https://www.instagram.com/p/Bp5fVofH0B2/?utm_source=ig_embed&utm_medium=loading
https://www.instagram.com/p/By5B3T3gZ9X/?utm_source=ig_embed&utm_medium=loading
https://www.instagram.com/p/B0YvJNRhLQ8/?utm_source=ig_embed&utm_medium=loading
https://www.instagram.com/p/B0R-EIcJCEA/?utm_source=ig_embed&utm_medium=loading
Risks of Dental Braces
While metal braces can transform a malocclusion into a beautiful smile, there are still risks associated. Traditional metal braces have a list of hazards, which many orthodontists don’t mention.
Here are some of the often unforeseen risks of dental braces, namely, traditional metal or ceramic braces.
Gum Problems
Unfortunately, traditional braces come with an increased risk for gingivitis and gum disease. This comes with inflammation of the gums, and gum recession.
While braces may help your teeth, they may not do the same for your gum line. It’s imperative to take good care of your gums while you have braces and watch for developing issues.
Teeth Concerns
The teeth are also a concern in traditional braces treatment. There is a danger of root resorption, where bone structures or a tooth’s roots begin to break down.
You may also notice white calcifications on teeth after your braces are removed—unfortunately, those can’t be corrected with teeth whitening.
Finally, braces can make brushing and flossing more difficult, which can lead to excessive plaque buildup and potential cavities.
Other Issues
Due to shifting of the upper and lower jaw, you are more likely to develop TMJ disorders if you have traditional braces. Heavy metal toxicity is also possible due to the metallic contents of braces.
Also, archwires may be coated in Teflon. This contains many chemicals that have been traced to hormonal imbalances and an increased risk of cancer. Long exposure to this material in braces can harm your endocrine and immune systems.
Dentists vs. Orthodontists for Braces
While general dentists are able to provide most types of orthodontic treatment, it’s usually better to go to an orthodontist. Orthodontists have completed 2-3 years of additional training to become specialists in treating malocclusions.
Also, if you can, begin bringing your child as young as two to a dentist and orthodontist who practices orthotropics. This will help guide the development of the child’s mouth and bite and prevent the need for serious malocclusion treatment.
An orthodontist will likely be more expensive than your general dentist, so that’s a factor to consider as you choose.
FAQs on Braces
How long does it take to move teeth with braces?
The length of your braces treatment depends on several factors: age, type of braces worn, whether expansion is needed, and any potential problems that may occur with the braces. Also, the severity of the malocclusion can determine how long treatment is needed to see lasting results.
Can I play sports with braces?
Yes, you can. Just be sure to wear a mouthguard, which I always suggest.
What happens if my wisdom teeth come in during or after my braces?
It’s important to communicate to your orthodontist about wisdom teeth coming in during your braces treatment. They can create a plan that doesn’t interrupt your care. If your braces are off and you notice your wisdom teeth coming in, keep wearing your retainer and book an appointment to see your dentist right away to avoid shifting teeth or decay.
Can I get braces for free?
While free braces are hard to find, there are a variety of discounted orthodontic programs accredited by the American Association of Orthodontists. Their list of approved schools can give you braces at a fraction of the cost—though the treatment may take longer as they learn.
When were braces invented?
Many ancient societies dreamed of ways to straighten teeth. In the 18th century, Pierre Fauchard made an early version of a palate expander, and soon another French dentist named Etienne Bourdet began removing teeth to fix overcrowding. Eventually, in 1880, J.N. Farrar pioneered the idea of using mild force in timed intervals to move teeth.
Key Takeaways: Dental Braces
Dental braces are an excellent solution for bite problems, overcrowding, and other common issues. The type of braces you choose can determine many factors, from length of treatment and risks to cost. After choosing your variety of braces, there are many foods to eat, brushing and flossing methods, and preventative measures that will help you to take care of them.
Be sure to consistently wear your retainer and to keep your dentist updated on any changes like shifting or wisdom teeth, even after your braces are off. Don’t forget to enjoy smiling, biting, and living malocclusion-free on the other side of orthodontic braces.
14 Orthodontic Treatments + How to Make the Most of OrthodonticsReferences
- Fleming, P. S., Proczek, K., & DiBiase, A. T. (2008). I want braces: factors motivating patients and their parents to seek orthodontic treatment. Community dental health, 25(3), 166-169. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/18839723
- Tang, E. L., & Wei, S. H. (1993). Recording and measuring malocclusion: a review of the literature. American Journal of Orthodontics and Dentofacial Orthopedics, 103(4), 344-351. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/8480700
- Ravaghi, V., Kavand, G., & Farrahi, N. (2015). Malocclusion, past orthodontic treatment, and satisfaction with dental appearance among Canadian adults. J Can Dent Assoc, 81(13), 1-6. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/26352521
- Tran, K., & Picheca, L. (2017). Orthodontic Treatment for the Management of Pain or Impacted Teeth in Patients with Malocclusion: A Review of Clinical Effectiveness and Guidelines. Abstract: https://www.ncbi.nlm.nih.gov/books/NBK519547/#
- Kassas, W., Al-Jewair, T., Preston, C. B., & Tabbaa, S. (2013). Assessment of Invisalign treatment outcomes using the ABO Model Grading System. Journal of the World Federation of Orthodontists, 2(2), e61-e64. Abstract: https://www.sciencedirect.com/science/article/abs/pii/S2212443813000234
- Schupp, W., Haubrich, J., & Neumann, I. (2010). Class II correction with the Invisalign system. J Clin Orthod, 44(1), 28-35. Full text: https://www.researchgate.net/publication/44631419_Class_II_correction_with_the_Invisalign_system
- Popowich, K., Nebbe, B., Heo, G., Glover, K. E., & Major, P. W. (2005). Predictors for Class II treatment duration. American journal of orthodontics and dentofacial orthopedics, 127(3), 293-300. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/15775943/
- Kataoka, K., Ekuni, D., Mizutani, S., Tomofuji, T., Azuma, T., Yamane, M., … & Morita, M. (2015). Association between self-reported bruxism and malocclusion in university students: a cross-sectional study. Journal of epidemiology, 25(6), 423-430. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4444496/
- Sauerheber, R. (2013). Physiologic conditions affect toxicity of ingested industrial fluoride. Journal of environmental and public health, 2013. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3690253/
- Noda, A., Nakata, S., Koike, Y., Miyata, S., Kitaichi, K., Nishizawa, T., … & Yokota, M. (2007). Continuous positive airway pressure improves daytime baroreflex sensitivity and nitric oxide production in patients with moderate to severe obstructive sleep apnea syndrome. Hypertension research, 30(8), 669. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/17917313
- Konturek, S. K., & Konturek, P. C. (1995). Role of nitric oxide in the digestive system. Digestion, 56(1), 1-13. Abstract: https://www.karger.com/Article/Abstract/201214
- Littlewood, S. J., Millett, D. T., Doubleday, B., Bearn, D. R., & Worthington, H. V. (2016). Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database of Systematic Reviews, (1). Full text: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD002283.pub4/abstract
- Moon, S. E., Kim, H. Y., & Cha, J. D. (2011). Synergistic effect between clove oil and its major compounds and antibiotics against oral bacteria. Archives of oral biology, 56(9), 907-916. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/21397894
- Andriekute, A., Vasiliauskas, A., & Sidlauskas, A. (2017). A survey of protocols and trends in orthodontic retention. Progress in orthodontics, 18(1), 31. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5632597/
- Azaripour, A., Weusmann, J., Mahmoodi, B., Peppas, D., Gerhold-Ay, A., Van Noorden, C. J. F., & Willershausen, B. (2015). Braces versus Invisalign®: gingival parameters and patients’ satisfaction during treatment: a cross-sectional study. BMC Oral Health, 15(1), 69. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4478712/
- Mikulewicz, M., Chojnacka, K., Woźniak, B., & Downarowicz, P. (2012). Release of metal ions from orthodontic appliances: an in vitro study. Biological trace element research, 146(2), 272-280. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3310133/
- Environmental Working Group, (2007). EWG assessment of EPA draft human health risk assessment for the teflon chemical PFOA. Retrieved from: https://www.ewg.org/research/ewg-assessment-epa-draft-human-health-risk-assessment-teflon-chemical-pfoa#.WkVkolQ-eCQ
- Suresh, M., Ratnaditya, A., Kattimani, V. S., & Karpe, S. (2015). One phase versus two phase treatment in mixed dentition: a critical review. Journal of international oral health: JIOH, 7(8), 144. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4588783/
 14 Orthodontic Treatments + How to Make the Most of Orthodontics
14 Orthodontic Treatments + How to Make the Most of Orthodontics