If your teeth and/or jaw are misaligned, it’s important to get orthodontic treatment in order to straighten your bite. Whether by traditional braces, Invisalign, or a mouthguard, all orthodontic appliances help straighten teeth or keep them straight.
Orthodontic care is a complex specialty branch of dentistry that requires additional education beyond general dentistry. If you’re a candidate for orthodontics, you may find that a successful treatment plan improves your self-confidence by improving your beautiful smile.
What kinds of treatments are available from an orthodontist?
I discuss available treatments and how to care for your orthodontic appliances. Plus, we’ll take a look at how to choose a great orthodontist and when to get started.
Why You Need Orthodontic Care + When to Start
Although it’s often thought of as a childhood need, orthodontic care is necessary for many adults, too. Here are some signs dentists look for to determine whether or not to suggest orthodontic treatment:
- Teeth crowding: Crowded teeth that can’t fit properly on the dental ridge; this is often caused by poor facial development before age 5
- Crooked teeth: Teeth that are tilted or twisted
- Overbite: Upper teeth too far forward that stick out above lower teeth (may be referred to as “retrognathism” or “buck teeth”; depending on severity, this can fit into either class 1 or class 2 malocclusion)
- Underbite: Lower teeth too far forward that create a “bulldog” look of the teeth, also called “reverse bite” (labeled as class 3 malocclusion, also called “prognathism”)
- Crossbite (edge to edge bite): When top and bottom teeth meet exactly and the top teeth don’t move slightly in front of the lower when teeth are closed
- Open bite: Back teeth meet and leave spaces between side or front teeth
- Spacing: For small kids, gaps between teeth are a good sign, but large spaces (from missing teeth or other issues) can be problematic for adults
- Impacted teeth: When teeth don’t emerge far enough out of the bone
- Poor aesthetics: When teeth aren’t aesthetically pleasing, it can affect self-confidence and require the need for orthodontic correction
- TMJ: Bite problems like one tooth hitting first can cause major pain in the TMJ and lead to chronic TMD
- Cavities, bad breath, and gum disease: Because misaligned or crooked teeth make it much harder to floss or brush your teeth, the oral microbiome can become overrun and lead to oral health problems like these
- Mouth breathing: You might breathe through your mouth because of a smaller-than-average airway at night from a misaligned bite, which can lead to everything from cavities to TMJ to symptoms of ADHD in children
These issues can affect children and adults alike.

Get Dr. B’s Dental Health Tips
You can’t be healthy without a healthy mouth. Sign up for my free newsletter and you’ll get my unconventional tips, starting with: If I had a cavity, here’s exactly what I’d do to reverse it.

When is the right time to first see an orthodontist?
Ideally, all children should get an orthodontic assessment between ages 2 and 5 to determine the need for any growth corrections. Treatment at that point will focus mostly on jaw and palate growth to ensure proper space for all teeth in the mouth.
Then, between 4-10 years old, any growth problems can be monitored and treated as needed. If growth has been corrected during the toddler years, you can cut down on the possibility your child will need braces or Invisalign.
After the age of 10, if there are additional corrections needed, a short course of clear aligners can be used (like Invisalign Express, meant for small, minor movements).
In orthodontics, this process is called Phase 1 and Phase 2 treatment.
This kind of early orthodontic intervention is key to the most effective treatment plans. The longer a child waits before having their orthodontic problems corrected, the more difficult (and expensive) the process will become.
You may have also heard the term “orthotropics” as it relates to oral and jaw growth. Orthotropics is a philosophy of orthodontic care for children that aims to correct growth issues as early as possible without tooth extractions.
It goes against some traditional views of Phase 1/Phase 2 treatment, where many dentists don’t typically recommend an orthodontic assessment before age five.
When done well, orthotropic treatment can help your child develop a properly shaped facial structure and jaw with less need for corrective care later. That’s why I recommend this option to my patients with very young children.
Didn’t get your teeth corrected with orthodontics as a kid? That’s okay! No one is too old for orthodontic treatment. There are always options, no matter your age.
Benefits of Orthodontic Treatment
Although it’s easy to avoid the orthodontist to save money or due to fear, there are some major benefits to a mouth full of straight teeth. These include:
- Increased self-esteem sporting a healthy smile
- Easier dental hygiene (it’s easier to brush and floss)
- Improved speech
- Reduced pain from TMD (TMJ pain)
- Reduced risk of sleep issues that can cause bruxism
- Reduced risk of tooth decay, bad breath, and gum disease
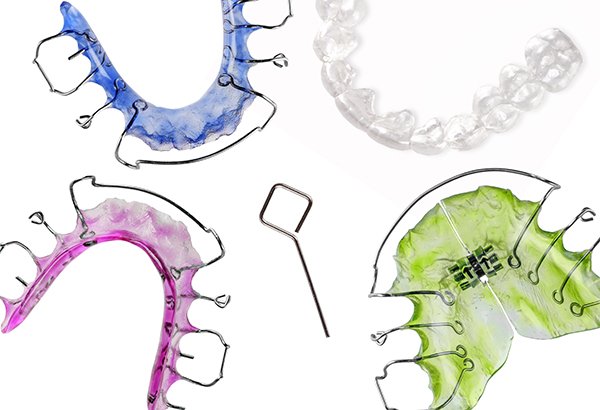
14 Orthodontic Treatment Options
Most often, people think of one thing when they hear “orthodontics”: braces. However, both metal braces and clear aligners like Invisalign are just two of the many appliances an orthodontist may create for you.
However, to help outline what you need to know about braces (including how to know which type is right for you), I created a video.
Now, let’s look at your options for orthodontic treatments and how each one works.
1. Clear Aligners (Invisalign, etc.)

For malocclusion (improper bite) where teeth are out of their proper position, clear aligners are often an excellent choice.
There are two major clear aligner brands that may be offered through your dentist: Invisalign and ClearCorrect.
This removable appliance is a modern solution to the problems of traditional braces (which I talk about below). But how does a clear aligner move teeth?
Clear braces like Invisalign work by using detailed scans of your teeth to determine a desired final result, then making aligners that gently move your teeth one week at a time. Each week, your teeth are moved more and more by the slightly differently shaped aligner.
I explain it to my patients as an elegantly choreographed movement over years. This can accomplish quite a bit of bite correction, according to research and case studies.
The pros of clear aligners, as opposed to metal braces, are extensive. Clear braces:
- Are removable
- Are more aesthetically pleasing
- Don’t leave white calcifications once removed
- Rarely lead to significant pain
- Can correct almost any problem metal braces can
- Are made of patented plastic that contains no BPA, BPS, latex, or gluten (for more information, here’s the most up-to-date MSDS sheet)
Brands that require dental oversight are significant expenses—a course of Invisalign, for instance, will probably run somewhere from $4000-6000. On the other hand, several companies (like SmileDirect Club, Candid, and SmileLove) now offer direct-to-consumer clear aligners. These are much less expensive, typically coming in at under $2,000.
For some bite corrections, direct-to-consumer aligners are perfectly appropriate (as long as you’ve consulted with your dentist to ensure you have no cavities, gum disease, or other oral issues).
But there are two cases in which you must get a course of aligners through your dentist: IPR and severely rotated teeth.
Interproximal reduction (IPR) is the process by which your dentist can create space between your teeth. If you need IPR, a course of at-home clear aligners will likely leave your teeth without the right amount of space to move as needed.
Severely rotated teeth are the second reason to avoid direct-to-consumer aligners. Professional aligners like Invisalign allow your dentist to add little attachments that let him or her rotate teeth that are rotated dramatically. I call these attachments “handlebars.”
In every case, it’s vital to get a dental cleaning and full exam before you start., including x-rays Tooth decay, gum disease, or other oral disease can render this orthodontic treatment useless if not identified and corrected.
Clear aligners may be a follow-up option for people who find they still have orthodontic issues after braces.
2. Metal Braces

The gold standard in orthodontics for many decades was metal braces. Utilizing metal wires and brackets, metal braces are fixed appliances that push and pull teeth into their proper position over time.
Braces are most effective for incredibly aggressive movements, where a great deal of space must be made. Once childhood is over, there is very rarely a justification for metal braces to be used instead of clear aligners, other than the more affordable cost.
One of the reasons metal braces might be needed is to complete orthodontic space closure, where teeth have been extracted and braces help to close the gap.
In orthotropics, braces may be used for very young children that have significant growth problems, usually to create space and widen the palate as the child grows.
I very rarely recommend patients get metal braces for a few specific reasons. There are significant cons to metal braces versus clear aligners, such as:
- Heavy metal toxicity
- Increased risk for gingivitis/gum disease
- Inflammation of the gums
- Gum recession
- Root resorption
- White calcifications on teeth after braces are removed (that can’t be corrected with teeth whitening)
- Difficulty brushing and flossing, which can lead to excessive plaque buildup
- TMJ disorders
- Pain and injury to cheeks, teeth, gums, and tongue
Before you opt for metal braces over aligners to save money, consider the far-reaching impact of braces. I’ve done both types of orthodontic correction and you can believe me when I say—aligners are the much more desirable choice, if you have the option.
3. Retainers
After major orthodontic treatment, your orthodontist will prescribe you a retainer. The purpose of a retainer is to keep teeth in their proper position without drifting back into their former spot.
Your teeth have a “memory” of where they used to sit before being moved. If you’re given a retainer and fail to use it for the first years after braces or aligners, your teeth will almost certainly move out of place.
Even after decades, I wear my retainer to bed almost every night to prevent shifting.
The first year after you finish orthodontic treatment, you should wear a retainer for 22 or more hours each day. After that, nighttime wear is encouraged.
There are removable and fixed retainers. Fixed retainers are also known as bonded retainers and are attached to the back of teeth with dental bonding. These are preferred generally for young people who are unlikely to keep up with their retainer without it being fixed into place.
There are two basic styles of retainers: metal (Hawley) and plastic (Invisalign). Both can theoretically be used forever unless your teeth move significantly.
Removable retainers can be stored and used at your discretion, but be sure to follow good practice for cleaning your retainers. Many creative products for “cleaning” retainers actually limit how long they’re useful.
4. Headgear

In the case of fast upper jaw growth, your orthodontist may recommend headgear. This removable device involves a strap around the back of the head which is fixed to a metal wire in front. This is sometimes called a “face bow.”
The upper teeth are held in place by the headgear so that their growth is slowed, while the lower jaw grows more rapidly.
Headgear seeks to prevent overbite caused by unequal jaw development.
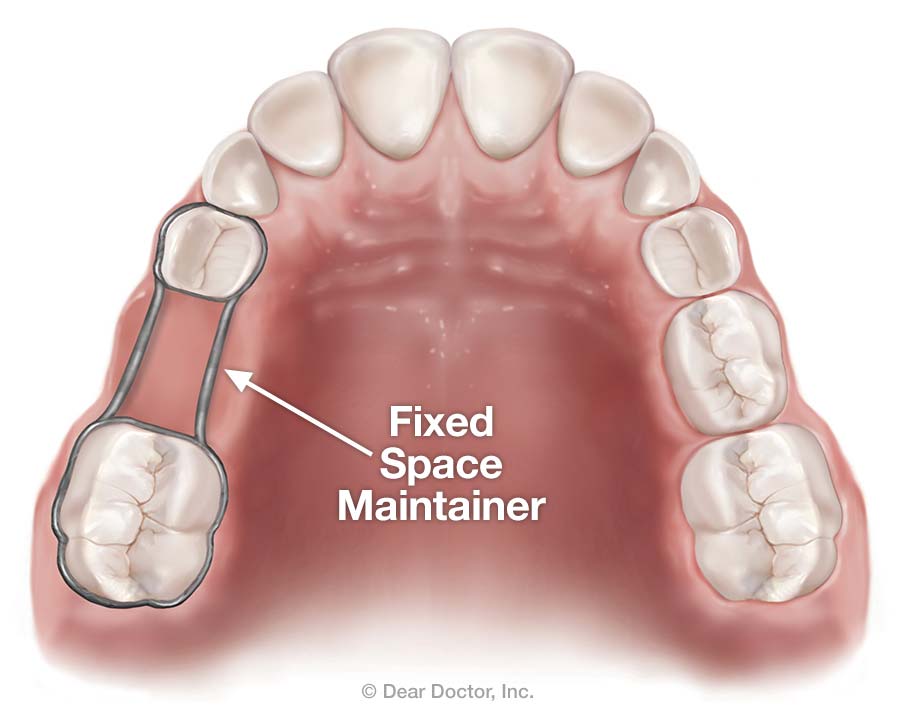
5. Space Maintainers
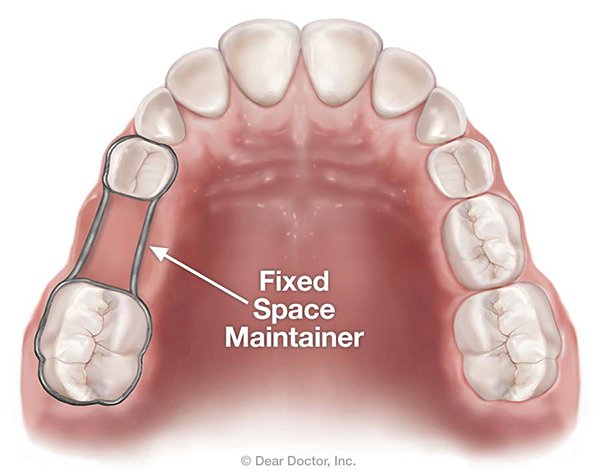
Used when baby teeth are lost too early, space maintainers can be either fixed or removable. They help to keep open space between baby teeth large enough for an adult tooth to come in. These are important because the shifting that could otherwise happen may result in crowded adult teeth if not addressed early.
Fixed space maintainers use metal wires, similar to braces, to keep the space open, connected to bands on the teeth on either side. A removable space maintainer are made with an acrylic base to sit over the jaw and may use metal or plastic wires between teeth.
6. Expanders

When the top palate doesn’t grow large enough to fit all of a child’s teeth, major orthodontic correction will be required later in life. Therefore, it’s important to use palatal expanders to prevent this problem.
Standard palatal expanders look similar to Hawley retainers, while expanders for “rapid maxillary expansion” are more heavy-duty (see the image above) and are fixed appliances.
Most palatal expansion is done in pediatric patients, but it can also be done in adults. However, this process is more uncomfortable for adults.
After a certain point in growth, the expander must be surgically attached within the mouth. This is called “Surgically Assisted Rapid Palatal Expansion (SARPE)”.
As you may imagine, this type of treatment isn’t a lot of fun for the patient, which is why supporting palatal growth early in life (as early as pregnancy) is so important. I encourage patients considering pregnancy or with very small children to ensure the child is getting plenty of vitamin K2, which is necessary for proper jaw and palate growth.
Negative side effects of palatal expansion include:
- Possible (minor) damage to gum tissue
- Pain or discomfort in jaws and teeth
- Problems articulating certain words or sounds
- Loss of buccal bone structure
7. Lip/Cheek Bumpers

Lip bumpers, sometimes referred to as cheek bumpers, serve a few different purposes:
- Provides space between the lips/cheeks and teeth to reduce pressure
- Holds back molars in place in order to lengthen the lower jaw’s arch
- Keeps primary/adult teeth from crowding forward on the bottom teeth before all baby teeth have been lost
- Preventing damage to the inside of the lips and cheeks
These bumpers are most effective when used while baby teeth are still present in the mouth and is a part of proper jaw and palate growth.
8. Archwires

With or without braces, orthodontic archwires (or “archwires”) are made in the shape of your dental arch and help to correct tooth position. “Initial” archwires are inserted at the very beginning of orthodontic treatment to fix major crowding and rotations.
Toxicity concern: Be aware that many types of archwires are coated with Teflon.
Teflon exposure is linked to many dangers, like:
- Hormone disruption
- Thyroid disease
- Low birth weight
- Chronic kidney disease (CKD)
- Cancer
Talk to your dentist/orthodontist about using an archwire material with your braces that’s free of Teflon to avoid these concerns. Don’t worry: there’s no evidence that any archwire material is any more or less effective in correcting crooked teeth.
9. Mouthguard

During sports and exercise, a mouthguard serves to protect teeth from traumatic damage. It can also cut down on the clenching many people experience while under physical exertion, potentially preventing or reducing TMJ pain.
Fitted mouthguards are an important part of any lifestyle that includes regular physical activity, especially high-intensity sports. Athletes without custom-fitted mouthguards experience over five times the dental trauma/injury than those who don’t use a mouthguard.
Remember, you only get one permanent set of teeth. No restoration lasts forever, so protect your teeth from damage with a mouthguard.
10. Special Fixed Appliances

If your toddler has an issue with tongue thrusting or thumb sucking, it’s important to step in to prevent orthodontic issues either. Sucking your thumb causes the palate and teeth to grow improperly (sort of like drinking from sippy cups).
Special fixed appliances can prevent these issues, but at a cost—they’re very uncomfortable, especially while eating. However, they are less expensive and less traumatic than having to get a full course of braces later in childhood.
11. Oral Splints

Suffer from pain in your temporomandibular joint (TMJ)? Your dentist might recommend an oral splint to relieve pain caused by what’s called a CR/CO discrepancy. This happens when your upper and lower teeth don’t meet correctly, which leads to TMJ pain.
An oral splint looks similar to a night guard for grinding, but it’s significantly more expensive to create because it uses “wings” that reset your jaw positions. This relieves pressure on your jaw muscles.
12. Sleep Apnea Oral Devices

There are multiple types of sleep apnea oral devices designed to support proper airway position during sleep. The most common of these are the:
- Mandibular advancement device (MAD)
- Night guard
- Tongue retention device (TRD)
You can get a non-custom TRD (like this one) but both night guards and MADs must be custom-fitted with your dentist or orthodontist.
These devices are often used in conjunction with a CPAP or APAP machine to help correct sleep apnea.
13. Serial Extraction
Some cases of crowded teeth indicate the need for serial extraction, typically in children younger than seven. Serial extraction involves removing up to four specific baby teeth, over many months’ time, to make better space for erupting adult teeth.
Multiple studies show that, when serial extraction is the only option, it frequently results in a positive outcome. However, this process is not preferred because it’s difficult for the child and still frequently requires the use of other orthodontics to keep teeth straight. It also more frequently leads to tongue thrusting than other treatment options.
To avoid this, work with an orthodontist earlier (around age 2) to correct growth issues before serial extraction is needed.
14. Orthognathic Surgery
Although it’s much rarer than other orthodontic treatments, orthognathic surgery can be used as a last resort for some patients. Typically, people in need of surgical orthodontic treatment have severe malformations of the jaw or palate and/or are too old for standard orthodontics to be effective.
Orthognathic surgery is expensive and not always covered by insurance since the necessity of it can be hard to “prove.” About 4-6 weeks after surgery, other orthodontic treatment will be needed.
This type of surgery is performed by an oral/maxillofacial surgeon and requires collaboration with your orthodontist for the best results.
How to Choose an Orthodontist
If you’re in need of orthodontics, choosing an orthodontist can feel daunting. There are a lot of questions to answer, like:
- Should my general dentist (DDS or DMD) perform my orthodontic treatment, or should I see a specialist?
- What hours does my orthodontist need to be open to accommodate my schedule?
- What dental insurance does my orthodontist accept?
- Is there additional financing offered?
- How convenient is the office to my home?
- Will the orthodontist oversee my treatment, or primarily his or her assistants?
As a general dentist, I’ve completed orthodontic treatment for many patients over my career. All general dentists can do these treatments, but orthodontists get additional education to specialize in orthodontics. For severe or complex cases, an orthodontist is typically preferred over a general dentist.
Overall, choosing an orthodontist is much like finding a good dentist. Ask people you know who have gone through braces, Invisalign, or other treatments like these. Find out who raves about their positive experience in this dental care specialty.
Most importantly, don’t feel rushed. You should feel heard and personally attended to when receiving orthodontic treatment. Be sure to stick with an orthodontist who makes you feel that way and has great online and in-person reviews to back up his or her experience.
Many people feel most confident about choosing a dentist who is a member of the American Association of Orthodontists (AAO). This organization retains over 19,000 members of licensed orthodontists in the United States, committed to a very high level of orthodontic care.
Good Oral Hygiene with Orthodontics
Your dental health is of supreme importance when using any type of orthodontics. One of the major reasons people struggle with braces, for instance, is that they make it more difficult to avoid plaque buildup.
Maintain good oral hygiene while undergoing orthodontic treatment by doing the following:
- Whenever possible, avoid decay-promoting foods. This includes the obvious, such as sugary desserts and soda, but also some unexpected culprits, such as breads, pastas, excessive fruits, and starchy veggies.
- Follow a diet rich in foods that promote healthy teeth and gums. A Paleo-like or ketogenic diet are ideal for remineralizing teeth and reducing gum inflammation.
- Brush your teeth in the morning, before bed, and 30-45 minutes after decay-promoting meals. It’s important to wait a little while after a starchy or sugary meal, but brushing your teeth regularly is important for orthodontic success.
- Floss every day. Most people don’t wake up excited to floss, but unchecked foods between teeth can wreak havoc with orthodontic appliances. Flossing with braces can be time-consuming, but it’s worth it—set aside time to make sure it happens.
- Avoid whitening toothpaste. Traditional whitening pastes are more abrasive than necessary, and their stain removal can leave your teeth unevenly white during orthodontic treatment.
- Use a toothpaste that supports remineralization. Fluoride toothpaste is the going standard, but there’s a better option: hydroxyapatite (Ha or NHa) toothpaste. This more natural remineralizing agent can help remineralize teeth and isn’t associated with the same side effects as fluoride. (Here’s my favorite; use code ASKTHEDDS for 10% off.)
- Don’t use alcohol-based mouthwash. It might sound counterintuitive, but conventional mouthwashes dry out your mouth and set the stage for the overgrowth of bad bacteria leading to decay and inflammation. (I like this oil pulling natural mouthwash instead.)
- Mouth tape every night. Taping your mouth shut at night to prevent nighttime mouth breathing is a great way to keep a handle on bad oral bacteria.
Taking Care of Orthodontic Appliances
As they’re expensive and vital to proper dental alignment, your appliances deserve a high level of care.
With fixed devices like braces, consider avoiding foods that can get stuck between teeth easily, like popcorn, corn on the cob, tough foods, taffy, or chewing gum.
Here are some tips for taking the best care of your removable orthodontic appliances:
- Keep them moist. Especially with Invisalign-type products, the worst thing to do is let your orthodontics get dried out.
- Avoid brushing plastic appliances. Invisalign, all retainers, mouthguards, oral splints, and sleep apnea devices can all develop microabrasions when brushed. Those abrasions make a home for bacteria to hang out, so avoid brushing your appliances (especially with abrasive toothpaste).
- Avoid denture cleansers. While it might sound great to disinfect your appliances using ADA-approved cleansers for dentures, the persulfate many brands contain can be harmful to your sensitive oral tissue.
- Soak them in baking soda when they’re not in use. Baking soda in water is a great cleansing agent that doesn’t pose harm to your orthodontic appliances.
- Once a week, soak your appliance in vinegar for 15 minutes, then thoroughly rinse it. Vinegar will add a deep clean for any plaque buildup your removable device might gather.
- If you’re concerned about the state of your device, talk to your dentist. Dentists and orthodontists have professional cleaning equipment right in the office that they can use for stubborn plaque buildup on orthodontic devices.
For the exact recipes I recommend for both baking soda and vinegar soaks, check out my DIY retainer cleaner.
History of Orthodontics
As long ago as ancient Egypt, straight teeth mattered for an attractive appearance. Etruscans, Romans, and French history all show record of primitive types of orthodontic treatment.
In 1901, the first orthodontics school was founded after decades of experimental treatments. The term “orthodontia” was used to describe this practice for many years.
Throughout the 20th century, orthodontists shifted their focus from simply straightening teeth to correcting the entire posture of the mouth’s structure through the growth process. It’s only in the last ¾ of a century that orthodontic treatment has approached what it looks like today.
FAQs on Orthodontics
When are you too old to get braces?
Ideally, a child will get an orthodontic assessment between ages 2-5, with treatment to support proper growth beginning within childhood years. However, one out of every five patients undergoing orthodontics is over the age of 18.
If you get braces or other orthodontic treatment as an adult, it will probably take longer than for a child. Not all changes can be completed without orthognathic surgery, and the oversight of a dentist is crucial if you’ve had any history of gum disease.
What’s the difference between an orthodontist and a dentist?
All orthodontists begin as general dentists. After dental school, orthodontists complete 2-3 years of additional schooling to specialize in orthodontia.
While they start out with standard dental education, orthodontists don’t offer general dental care, such as cavity restorations, cleanings, or whitening.
Are metal braces better than clear aligners?
Metal braces come with several cons that clear aligners don’t, like an increased risk for gum disease or soft tissue damage. However, metal braces are necessary in some cases that require significant force and “pulling” of teeth.
Overall, clear aligners are preferred in the majority of cases because of the risks involved.
How can I prevent my child’s need for orthodontics?
I teach my patients prevention whenever possible, because it’s always less expensive and less painful to prevent problems before they happen. Orthodontics is no different.
There are several ways to prevent the need for orthodontic treatment. While these aren’t a guarantee, all will support proper growth of oral structures and straight teeth:
- Get plenty of vitamin K2 during pregnancy through foods and/or supplements, which is crucial to the development of the bottom ⅓ of the face
- Avoid prolonged use pacifiers (after age one)
- Breastfeed as often and for as long as you can (at least one year is optimal)
- Toss out sippy cups or minimize their use as much as possible
- Supplement with cod liver oil
- When your pediatrician says your child is ready, transition from pureed foods to chewable, remineralizing foods like crunchy celery or small pieces of meat
- Have your pediatrician check for tongue ties and have them clipped if found
Why do so many people need braces?
Weston A. Price’s revolutionary research, although flawed in many ways, was a great picture of the modern need for orthodontics that wasn’t needed in the past. In short, the foods that were easier to produce and lasted longer on shelves were also foods that are devoid of vital nutrients like vitamin K2 (which he dubbed “Activator X”).
When these foods replaced the more common Paleo-like diet, the maxillofacial structure began to suffer in just a generation or two. However, when a diet high in healthy fats, vegetables, grass-fed animal proteins, cheeses, nuts, seeds, and fruits was employed, Price recorded the results: a reversal of orthodontic issues (not to mention tooth decay!).
In general, it is the modern diet that has changed the value of nutrition our bodies evolved to need, and that includes our facial structure and teeth.
If I don’t mind the way my smile looks, do I still need orthodontics?
Straight teeth may improve your self-confidence, but they’re far from simply an aesthetic change. Malocclusion of the teeth can lead to many issues, including TMJ pain, grinding/clenching of the teeth, tooth sensitivity, speech issues, and more.
If your teeth are crowded, twisted, or otherwise show placement issues, I recommend you see an orthodontist, even if the visual appearance doesn’t bother you.
How long does orthodontic treatment take?
Treatments range in the time they need to be effective, but most orthodontic treatments take somewhere between 1-5 years to complete. Factors that affect this are levels of treatment required, patient’s age, and preferred method.
Once I have braces, do I still need to see my orthodontist?
Your orthodontist will work with you to create a retainer and monitor your treatment immediately after your braces are off. After your first 1-2 follow-up appointments, you shouldn’t need to continue visiting the orthodontist. However, bi-yearly teeth cleanings are important as part of keeping your straight smile healthy!
References
- Suresh, M., Ratnaditya, A., Kattimani, V. S., & Karpe, S. (2015). One phase versus two phase treatment in mixed dentition: a critical review. Journal of international oral health: JIOH, 7(8), 144. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4588783/
- Kassas, W., Al-Jewair, T., Preston, C. B., & Tabbaa, S. (2013). Assessment of Invisalign treatment outcomes using the ABO Model Grading System. Journal of the World Federation of Orthodontists, 2(2), e61-e64. Abstract: https://www.sciencedirect.com/science/article/abs/pii/S2212443813000234
- Schupp, W., Haubrich, J., & Neumann, I. (2010). Class II correction with the Invisalign system. J Clin Orthod, 44(1), 28-35. Full text: https://www.researchgate.net/profile/Werner_Schupp/publication/44631419_Class_II_correction_with_the_Invisalign_system/links/0f317539dd7958ed92000000/Class-II-correction-with-the-Invisalign-system.pdf
- Mikulewicz, M., Chojnacka, K., Woźniak, B., & Downarowicz, P. (2012). Release of metal ions from orthodontic appliances: an in vitro study. Biological trace element research, 146(2), 272-280. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3310133/
- Azaripour, A., Weusmann, J., Mahmoodi, B., Peppas, D., Gerhold-Ay, A., Van Noorden, C. J. F., & Willershausen, B. (2015). Braces versus Invisalign®: gingival parameters and patients’ satisfaction during treatment: a cross-sectional study. BMC Oral Health, 15(1), 69. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4478712/
- Gauthier, C., Voyer, R., Paquette, M., Rompré, P., & Papadakis, A. (2011). Periodontal effects of surgically assisted rapid palatal expansion evaluated clinically and with cone-beam computerized tomography: 6-month preliminary results. American Journal of Orthodontics and Dentofacial Orthopedics, 139(4), S117-S128. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/21435529
- Stevens, K., Bressmann, T., Gong, S. G., & Tompson, B. D. (2011). Impact of a rapid palatal expander on speech articulation. American Journal of Orthodontics and Dentofacial Orthopedics, 140(2), e67-e75. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/21803236
- Garib, D. G., Henriques, J. F. C., Janson, G., de Freitas, M. R., & Fernandes, A. Y. (2006). Periodontal effects of rapid maxillary expansion with tooth-tissue-borne and tooth-borne expanders: a computed tomography evaluation. American journal of orthodontics and dentofacial orthopedics, 129(6), 749-758. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/16769493
- O’Neill, J. (2009). Do lip bumpers work?. Evidence-based dentistry, 10(2), 48. Full text: https://www.nature.com/articles/6400651
- Mohamed, K., Kumar, V. A., Padmanabhan, T. V., Deora, N., & Mohan, S. (2012). Cheek bumper prosthesis for a patient with a neurofibromatous lesion in the left cheek. Journal of Prosthodontics: Implant, Esthetic and Reconstructive Dentistry, 21(6), 482-486. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/22913839
- Farronato, G., Maijer, R., Carìa, M. P., Esposito, L., Alberzoni, D., & Cacciatore, G. (2011). The effect of Teflon coating on the resistance to sliding of orthodontic archwires. The European Journal of Orthodontics, 34(4), 410-417. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/21478301
- Fei, C., McLaughlin, J. K., Lipworth, L., & Olsen, J. (2009). Maternal levels of perfluorinated chemicals and subfecundity. Human Reproduction, 24(5), 1200-1205. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/19176540
- Melzer, D., Rice, N., Depledge, M. H., Henley, W. E., & Galloway, T. S. (2010). Association between serum perfluorooctanoic acid (PFOA) and thyroid disease in the US National Health and Nutrition Examination Survey. Environmental health perspectives, 118(5), 686-692. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2866686/
- Fei, C., McLaughlin, J. K., Tarone, R. E., & Olsen, J. (2007). Perfluorinated chemicals and fetal growth: a study within the Danish National Birth Cohort. Environmental health perspectives, 115(11), 1677-1682. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2072850/
- Shankar, A., Xiao, J., & Ducatman, A. (2011). Perfluoroalkyl chemicals and chronic kidney disease in US adults. American journal of epidemiology, 174(8), 893-900. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3218627/
- Barry, V., Winquist, A., & Steenland, K. (2013). Perfluorooctanoic acid (PFOA) exposures and incident cancers among adults living near a chemical plant. Environmental health perspectives, 121(11-12), 1313-1318. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3855514/
- Jian, F., Lai, W., Furness, S., McIntyre, G. T., Millett, D. T., Hickman, J., & Wang, Y. (2013). Initial arch wires for tooth alignment during orthodontic treatment with fixed appliances. Cochrane Database of Systematic Reviews, (4). Full text: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD007859.pub3/full
- Kjellgren, B. (2007). Serial extraction as a corrective procedure in dental orthopaedic therapy. The European Journal of Orthodontics, 29(suppl_1), i37-i50. Full text: https://academic.oup.com/ejo/article/29/suppl_1/i37/558043
- Almeida, R. R. D., Almeida, M. R. D., Oltramari-Navarro, P. V. P., Conti, A. C. D. C. F., Navarro, R. D. L., & Souza, K. R. S. D. (2012). Serial extraction: 20 years of follow-up. Journal of Applied Oral Science, 20(4), 486-492. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3881831/
- Khechoyan, D. Y. (2013, August). Orthognathic surgery: general considerations. In Seminars in plastic surgery (Vol. 27, No. 03, pp. 133-136). Thieme Medical Publishers. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3805731/
- Price, W. A. (1939). Nutrition and physical degeneration. A comparison of primitive and modern diets and their effects.,(Paul B. Hoeber Inc.: New York). Retrieved from: https://books.google.com/books?hl=en&lr=&id=-ktYCwAAQBAJ&oi=fnd&pg=PT8&dq=weston+a+price+1939&ots=4JR4NqkF0P&sig=FAezQzb34V_WmNtWOaS4CxS1bO0#v=onepage&q=weston%20a%20price%201939&f=false
 The Real Cost of Dental Insurance: Best Plans, Myths, and Benefits [2020]
The Real Cost of Dental Insurance: Best Plans, Myths, and Benefits [2020]
{kind=link}